
Translate this page into:
Crossing the Line to Electronic Medical Records in Subsaharian Africa: An Obstetric and Neonatal Information System with Perinatal Indicators Dashboard
*Email: mamourmb@yahoo.fr
Abstract
Objectives:
This study reports our experience in the use of a perinatal electronic medical record, E_Perinatal, by giving examples of its potential for the analysis of clinical data and the involvement of the indicators produced in the improvement of Emergency Obstetric and Neonatal Care in Africa.
Methodology:
This is a study that was conducted in the scenario of a Level II Health Centre in Senegal. The methodology of the study followed the following steps: an inventory of the use of electronic tools in labour wards in Senegal, an exploratory survey of the scenario of obstetric and neonatal care, simultaneous elaboration of an electronic medical record in obstetrics and neonatology and selection of obstetric and neonatal care indicators to automatically generated and implement the information system. The recording was retrospective and continuous from January 2015 to December 2016.
Results:
This database automates the storage of obstetric data, including antenatal care, obstetric ultrasound, hospital admissions, prescribing, etc., providing easy access to patient data from anywhere in the hospital, produce timely reports and graphs to refer to clinician correspondents, store and electronically transfer birth data to authorities, and store data for ad hoc queries and search statistics.
Conclusion:
E_Perinatal has demonstrated in a scenario of an intermediate health facility its usefulness and ease of use. Scaling up in a developing country will help to better understand the real problems and help to reduce maternal and neonatal mortality.
Keywords
Electronic Medical Record
E_Perinatal
Indicators
Health Information System

Introduction
A database is a structured and organized set that allows large amounts of information to be stored in order to facilitate their use (adding, updating, searching and possibly analysing).
Today, computing is not only a valuable aid for health care providers; it is at the heart of modern medicine, a medicine that requires information sharing between health system stakeholders and the patient in order to improve care, coordination and continuity of care.
Through the medical record, large amounts of information are generated daily by medical activities. This information is recorded in essentially textual documents, images and files whose mode of access and exploitation are mainly done manually and therefore difficult to reuse and share because of their structural heterogeneity.
To keep these millions of information collected, processed, analysed and exchanged, databases are required, which necessarily implies computerization of the patient’s record.
While computerization of the medical record isincreasingly evolving in western countries, it is slow to start in our regions; just from a chronological point of view, several decades separate us. In 2006, an informal survey conducted in fifteen Francophone African countries through the coordination of the Telemedicine Network in French-speaking Africa confirmed that there was no hospital information system integrating the management of medical information1.
In a developing country where maternal mortality is still high, computerized information on pregnancy and birth is important for assessing the quality of maternal and newborn care. If reliable tools are available to continuously evaluate the prenatal period, childbirth and newborn care, these will allow health care managers to monitor the quality and impact of their actions to improve health care.
Several medical data management systems are commercially available. Their relatively high cost led us to develop this personalized perinatal database using FileMaker Pro Advanced Inc.
This study reports our experience of using this platform by giving examples of its remarkable potential for analysing clinical data and the implication of the indicators produced in the improvement of Emergency Obstetric and Neonatal Care.
Methodology
This is an interdisciplinary applied research study between Medicine, Information and Informatics.
The health system in Senegal is based on 3 main types of health facilities: health posts, level 1 and 2 health centres, and hospitals.
This study was conducted in the scenario of a Level 2 Health Centre in Senegal. Level 2 health centres are facilities that do not have the hospital level but perform surgical procedures.
The recorded clinical data were obtained from the paper records of all obstetric admissions. Obstetricians and Gynaecologists, Neonatologists and Computer Scientists carried out the compilation of data for the automated calculation of indicators and their transcription to a standard in electronic form.
The methodology of the study followed the following three steps:
Assessment on the use of electronic tools in labour wards in the Senegal;
Exploratory survey of the obstetric and neonatal scenario;
Simultaneous development of an Obstetric and Neonatal Electronic Medical Record (EMR) and selection of indicators for obstetric and neonatal care to be automatically generated.
Initial Evaluation
We conducted an assessment of obstetric data collection of all Obstetrics facilities in Dakar, the capital of Senegal (public and private) and in all 13 regional hospitals in the country.
Definition of Variables
This step consisted of choosing the administrative and medical variables necessary to build a Perinatal Electronic Medical Record.
Transcription of the Values of the Manuscript to the Computer
The aim was to translate the data recorded on the paper version of the file into a specific electronic format. Since the structures did not yet have an integrated electronic recording system, the information was entered without a predefined structure. As a result, a set of data was deemed vital to automatically generate the selected indicators. These include: patient profile, caesarean indicators, and maternal and neonatal data for each admission.
Identification and Definition of Maternal and Neonatal Health Indicators
This is the definition of the most appropriate indicators for comparing the quality of obstetric and neonatal care, as well as the corresponding formulas and calculations for each indicator. Those of the World Health Organization met the criteria chosen.
Implementation of the Information System
We then had to find specific software for the collection, entry, storage and analysis of obstetrical data. Software is capable of composing the Electronic Medical Record and automatically generating indicators on the health of mothers and newborns. FileMaker Pro was chosen for this.
Installing Prototypes for Testing
The Electronic Medical Record so named E-Perinatal was tested in a reference health centre. The data used here comes from this centre.
This consisted of a continuous retrospective and prospective registration of patients’ records admitted for delivery from January 2015 to December 2016.
Results
Initial Assessment
All facilities visited had paper files. Only two structures one in Dakar, the capital of Senegal and one in Saint-Louis, 250 km from the capital, had been using recording software since 2011.
In all health facilities, each obstetric admission was the subject of a single paper file which is archived without a specific order at the patient’s exit.
The archive rooms were usually makeshift spaces, in cramped, unaerated and moist areas. Sometimes these archival spaces were open.
We found computers in most of the structures, placed in the offices of service managers (managers, doctors) and used for Internet browsing.
All structures provided monthly, quarterly and annual reports but these were limited to descriptive data (count).
The Perinatal Information System
E_Perinatal was designed using the Filemaker Pro Advanced software. FileMaker a database management software developed by an Apple subsidiary called FileMaker Inc. (formerly Claris). It runs on Mac OS X and Windows, either peer-to-peer networking or Client-server mode with “FileMaker Server”.
Access to the database is done using an account name and a password.
The terms module, folder, and table refer to a structure to organize and group data according to common characteristics or principles: abortion’s table or module for example.
The nucleus of this perinatal information system is the patient’s administrative record, containing her/his contact information, civil and family information and her/his background. To this nucleus, other tables are linked to capture all the information related to patient’s care during the stay in the hospital: follow-up of pregnancy, consultations, hospitalization, admission (child birth, ectopic pregnancy, abortion or other admission). There are also links to prescription module, an agenda (appointment management), a module for infertility management, specific modules for management of sexual abuse, HIV/ AIDS patients, a module for writing operational reports, an ultrasound module incorporating the growth curves of the Intergrowth 21st study, colposcopy and hysteroscopy modules.
The Neonatal file is related to the Childbirth file for the care of hospitalized new-borns and their outcome as well as specific care such as Kangaroo cares.
Queries and Reports Generated
Here we present some features of E_Perintal.
Medical Unit Summary (MUS)
Upon discharge from hospital, all admissions are subject to MUS containing the items recommended for discharge as well as the minimum European file: Hospital identification, file number, sex, age, marital status, and place of Residence, month and year of admission, length of stay, discharge status, main diagnosis, other related diagnoses, surgical and obstetric procedures, other significant interventions.
Depending on the type of admission (childbirth, abortion, ectopic pregnancy, gynaecological or pregnancy pathology), specific information supplemented the MUS file.
Notification of Obstetric Diagnosis and Complications
For each patient, one or more diagnoses may be attached to the admission. These diagnoses are selected from a linked table whose records are the categories of the Tenth International Classification of Diseases (ICD 10).
Some diagnoses are automatically recognized by the system as major obstetric complications as defined by the World Health Organization2.
These 7 complications known as major obstetrical complications are haemorrhage (antepartum and postpartum), prolonged or obstructed labour, postpartum septicaemia, complications of abortion (spontaneous or induced), severe preeclampsia and eclampsia, ectopic pregnancy and uterine rupture.
For example, for the study period, Figure 1 shows the severe obstetric complications recorded.

- Major obstetric complications recorded from 1/1/2015 to 31/12/2016.
Classification of Caesarean Sections
In 2014, the World Health Organization (WHO) conducted a systematic review of the experience of users of the Robson classification to assess the advantages and disadvantages associated with its adoption, implementation and interpretation, and to identify obstacles, facilitating elements and potential adaptations or modifications3. Among the recommendations was: “Health care facilities should use the Robson classification system for women hospitalized for childbirth.”
E_Perintal using the following parameters systematically recorded for each patient automatically generates this classification: parity, single or multiple pregnancy, presence of previous caesarean delivery, presentation, onset of labour, and gestational age at delivery.
Statistics
The statistical component is a real dashboard that allows seeing the trends of admissions, their mode (transferred or coming from the home) over a period chosen between two dates, a year or all of the registrations.
Each admission category is detailed on another sheet upon request. For example, deliveries are detailed according to the mode (vaginal, caesarean, vacuum, forceps), type of pregnancy, foetal presentation, birth weight, episiotomy or tearing, epidural anesthesia...
Notification of Maternal Deaths
Each death in the structure is subject to an audit in which the parameters of the process that led to the death are recorded. The cause of death is established as a direct, indirect, non-obstetric or unknown obstetric cause as shown in Figure 3 for the study period. The analysis of deaths goes further and makes it possible to classify them according to the cause, the specific lethality of each obstetric complication...

- Annual evolution of births between 2015 and 2016 (Figure 2A) and changes in delivery patterns (Figure 2B) displayed by the pop-up on a semi-logarithmic curve.
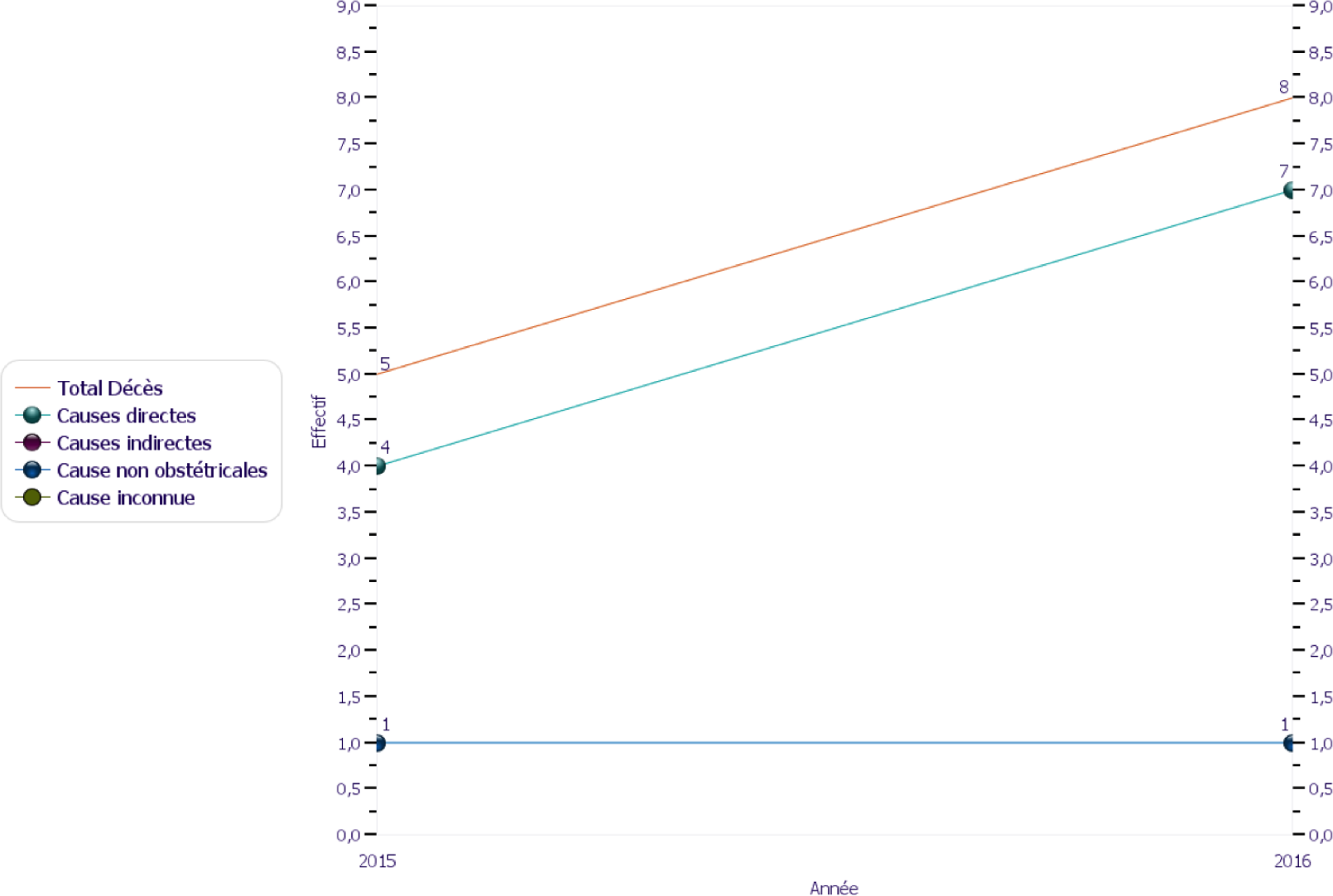
- Evolution of deaths by cause.
Discussion
E_Perinatal is business software as well as a registry for perinatal information.
Why using Filemaker?
Several medical data management systems have been developed and are commercially available4–11. E_Perinatal is an Electronic Medical Record (EHR) client-server system created using FileMaker. FileMaker was the only application with the necessary set of tools: a client/server application that works in a wireless local area network that could run on Windows or Mac OS laptops, mobile iOS devices (iPad and iPhone), and a doctor who had expertise from FileMaker. FileMaker is an excellent, cost-effective tool for making databases. It runs on both Macintosh and Windows systems, and is the best-selling database for both platforms. FileMaker databases can be shared simultaneously among multiple users, whether Mac or Windows or kept as a single user. FileMaker databases can also be viewed on iPhone and iPad using the FileMaker Go app connection. However, even if FileMaker is really easy to use (especially compared to Microsoft SQL or Access), designing a more complex database system still requires analytical skills and design expertise. The LAN allows access to the database system from each workstation in the centre. The system itself provides quick access to all patient data (with access rights) and processing information, screenshots of the plan and medical documentation.
The system allows a quick query on all the patient’s medical information. All data are readily available during the follow-up examination and are accessible at any time from any location of the service.
The attending physician has more information at hand and can focus on the patient to provide a better service
Collection and Research
In a previous evaluation study of Emergency Obstetric and Neonatal Care in our department, only 8.1% of the expected complications were actually recorded and managed. The comments indicated that the low percentage of satisfied needs was probably due to the fact that obstetric complications were not properly recorded. In such cases, it is desirable to examine how health facility records are maintained. They were not always properly maintained and it happened that a complication occurred and motivated care without being notified. However, the only complications recorded by supervisors are those recorded on the header of the file.
Several solutions have been proposed to alleviate this problem: recording of complications 24 hours a day, computerization of medical records, creation of a register of complications, etc. In addition, staff training or supervision of record keeping eventually reduces under-reporting2.
Forward-looking collection provides complete, accurate and valid data. Clearly organized and structured data entry and continuous control scripts ensure the quality of data collection. This is what E_Perinatal does.
Complex query scripts make it easy to retrieve large sets of data. These datasets are processed for predefined statistical analyses. All data can be imported to Excel spread sheets or Statistical Package for Social Science (SPSS) for in-depth statistical analysis.
The database serves as an information base for scientific matters, integrating all relevant medical and technical information into a single system.
Healthcare facilities can benefit from the implementation of their own research and development software. By consulting with local FileMaker developers, hospitals that also conduct research, can create custom database software that allows them to store critical information and results, as well as share this information with other doctors in the network. By doing this, health care providers can create a community that is at the forefront of research and innovation in their field, and also inform colleagues doctors and nurses about the latest data available in the field. This can help foster an innovative and committed organization for success.
Detailed and regular analysis of indicators of care, complications and deaths can improve practices and improve the quality of patient care.
Data Management - Data Manager
In addition to developing and implementing the software, the adoption of data management (data entry) in the daily workflow is crucial. Depending on the amount of data as well as the complexity of the database system, a dedicated data manager or administrator is required 12. If no additional staff can be allocated for this purpose, at least one coordinator is required to organize the input of the data and adapt the workflow to the existing workforce.
This task is often attributed to the physician who created and implemented the database.
A key aspect of the sustainability of E_Perinatal is to ensure that there is a local technical team capable of solving all the problems that arise and performing routine maintenance. At each stage of the installation, doctors and technicians of the health facility participated in the project and learned on the job. Several dedicated training sessions were organized to introduce users to the use of E_Perinatal.
Outlook
As this experience has proved useful, it is planned to share this experience with the shareholders of the perinatal health system (obstetricians and gynaecologists, midwives, etc.) and implement it in a university hospital and a private clinic in the near future.
Once feasibility has been identified at the level of these facilities, we will advise the administrative authorities for scaling up.
The solution can be used on iOS applications such as iPhone and iPad, and its use is even possible in remote areas not served by the electrification network.
Ultimately, the data will be more comprehensive with better visibility of obstetric complications and more targeted and effective action.
Conclusion
To keep millions of information collected, processed, analysed and exchanged, databases are required, which necessarily implies computerization of patient’s record. E_Perinatal has demonstrated in a scenario of an intermediate health facility its usefulness and ease of use. Scaling up in a developing country where maternal and neonatal mortality is still high will help to reduce it, to better understand the real problems that have so far been identified only on piecemeal data.
References
- Mise en place d’un Système d’Information Hospitalier en Afrique Francophone: Cinz@n, étude et validation du modèle au Mali In: Thèse Santé publique et Recherche Clinique]. Aix-Marseille II : Université de la Méditerranée. 2010.
- [Google Scholar]
- Déclaration de l’OMS sur les taux de césariennes. 2015. Disponible à http://apps.who.int/iris/bitstream/
- [Google Scholar]
- Database management for a gynecologic oncology service. Gynecol Oncol. 1990;38(3):431-6.
- [CrossRef] [Google Scholar]
- Development and integration of the Oncological Documentation System ODS. Zentralbl Gynakol. 2001;123(8):444-9.
- [CrossRef] [PubMed] [Google Scholar]
- An electronic medical record system with direct data-entry and research capabilities. Int J Radiat Oncol Biol Phys. 1992;24(2):369-76.
- [CrossRef] [Google Scholar]
- Presentation of an oncological database adapted for head and neck cancer. Laryngorhinootologie. 2002;81(12):875-81.
- [CrossRef] [PubMed] [Google Scholar]
- Prognostic index for patients with parotid carcinoma: international external validation in a Belgian-German database. Cancer. 2009;115(3):540-50.
- [CrossRef] [PubMed] [Google Scholar]
- A computerized database for managing otorhinolaryngologic oncology patients. Acta Otorhinolaryngol Ital. 1998;18(3):155-63.
- [PubMed] [Google Scholar]
- adonco database–six years’ experience with the documentation of clinical and scientific data on patients with head and neck cancer. In Vivo. 2010;24:603-6.
- [PubMed] [Google Scholar]




