
Translate this page into:
Sexual Behaviour, Knowledge and Use of Contraceptives Among Undergraduate Students
*Email: enwose@csu.edu.au
Abstract
The reproductive health of young adult women is integral to the well being of a society. The independence, lifestyle and sociocultural environment within an undergraduate institution predisposes to sexual behaviour that has become a serious concern in Nigeria and the global community at large. Previous studies have shown that there is significant or sufficient knowledge of contraceptives, especially among the youth in universities. This study is aimed at determining data on the sexual behaviour, knowledge and use of contraceptive, with a view to what may be known and unknown among undergraduate university students in Delta State from the contextual point. The methodology employed for this study was a narrative literature review approach. In order to guide the researcher, four composite focus of inquiry included (1) healthy and risky sexual behaviours, (2) contraception, (3) determinants of choice and use of contraceptives, and (4) knowledge and use of contraceptives among undergraduate students. The finding of this study indicates abundance of knowledge about sexual health. However, two themes are of particular mention needing further attention. Firstly, characteristics of being sexually healthy seem to be mixed up with healthy sexual behaviour. Secondly, contraception usage does not seem to match acclaimed knowledge, which translates to risky sexual behavior. How the undergraduate girls are successfully preventing pregnancies in order to maintain uninterrupted education also seems to remain a gap in the literature. Further research will benefit to provide adequate information on these two themes.
Keywords
Behavioural Change Wheel
Healthy Sexual Behaviour
Sexually Healthy

Introduction
Sexual activities among young ones are on the increase all over the world with a trend towards early onset. Many of the young adults have initiated their first sexual activity in their adolescent age. In Nigeria, up to 6% of all sexually active adolescent girls may have been pregnant and engaged in induced abortion1. Sexual behaviour has been defined as any activity that induces sexual arousal and two major determinants have been noted to be (1) genetics2 and (2) degree of sociocultural regulation exerted on an individual to express sexuality3,4.
The contraceptive is a birth control tool to prevent pregnancy and Sexually Transmitted Diseases (STD) acquisition. Contraceptives are relatively accessible and affordable, with numerous types or options being available. Yet, incidence of unplanned pregnancies and STDs are still high5. Indeed, teenage pregnancies is a global issue and probably highest in sub-Saharan Africa6. While contraceptive remain a preventive measure for both STD and teenage pregnancy, it also known that several factors influence adolescents’ sexual behaviour in relation to the use of contraceptives7–10. Notably, these factors include, but are not limited to peer- sociocultural pressures to engage in premarital sex11, albeit without commensurate education against the consequences.
Associated with the problem of unwanted pregnancies has been the concept of unmet needs of family planning. A study on sexual behaviour and contraceptive usage has been done in Delta State University (Figure 1)5. However, that study included staff and students without delineation of student subpopulation for special evaluation. It is against this background that this study seeks to examine the literature on sexual behaviour, knowledge and contraceptive use among undergraduate female students in a University in Delta state of Nigeria. The objective is to translate the undergraduates’ birth control practice to the non-university community.
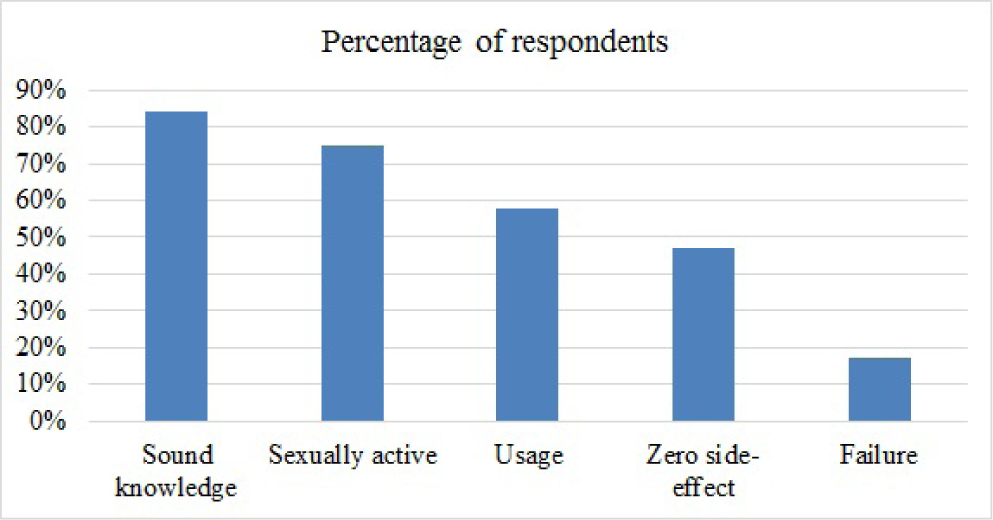
- Reported data on contraceptive usage from Delta State university community5.
Narrative Review
Methodology
The research methodology employed for this study was a narrative literature review approach. Firstly, four composite focus of inquiry were defined to include 1. Healthy and risky sexual behaviours, 2. Contraception, 3. Determinants of choice and use of contraceptives, and 4. Knowledge and use of contraceptives among undergraduate students. Secondly, a narrative inquiry to understand the literature as narratives was performed with a view to developing a story that will substantiate or support the need for future research. Literatures on the four composite focus were searched, albeit not in a systematic review paradigm, google scholar and PubMed amongst others.
Sexual Behaviour
Sexual behaviour is any activity between two persons that induces sexual arousal12. Sexual behaviour is defined as a person sexual life. Sexual behaviour as it pertains to sex includes courtship, masturbation, estral display and the mating act13. It is one aspect of the total pattern of reproductive behaviour in animals14,15, including all responses directly associated with genital stimulation and copulation. In the animal, much of the behaviour is visual including posture, feather fluffing, and tail carriage; Some of it is auditory, especially in cats, but chemical communication via pheromones is the clincher12.
Sexual behaviour in humans has been defined as the manner in which human’s experience and express their sexuality16. It encapsulates how people engage in sexual acts in a variety of ways including but never limited to masturbation, romance, and sexual intercourse (which again include various forms such as anal, oral, or vaginal; as well as penetrative ornon-penetrative sex). Sexual behaviour also includes any conduct and activity intended to arouse the sexual interest of another. For instance, beside romance, modes of dressing, personal interactions between individuals and use of body perfumes may be deliberate to seduce a person of interest. In this context, sexual activity or behavior is appreciated to possess cognitive, emotional, and health aspect17. Of particular importance in this narrative is the health aspect, which can be delineated dichotomously as either healthy or risky sexual behavior18.19.
The Healthy Sexual Behaviour
Sexual activity is a normal physiological function and a person’s sexual behaviour is considered healthy if it can be controlled. Sexual Behaviour (SB) develops over time from childhood; and at a particular time of a person’s life, SB can be termed appropriate/healthy or inappropriate/unhealthy19. The characteristics of a healthy sexual behaviour can grouped into communication, relationship, and self-worth. Others are education and values20. However, it is noteworthy that the team from Minnesota has described these characteristics of ‘sexually healthy’, which is probably a misnomer.
An adult with a healthy sexual behaviour interact with partner and considers all stakeholders (family and friends amongst others) in appropriate and respectful manner. This include appropriately expressing desires to have sex, or not to have sex; as well as negotiating sexual limits and accepting refusals of sex without hostility or feeling insulted20. Relative to rape and sexual assault, healthy sexual behaviour involves being consciously and conscionably sensitive to the feelings of other persons’ nonverbal cues and boundaries21,22.
A person with healthy sexually behaviour develops friendship with any gender without necessarily having any sexual agenda. In sexual relationships, healthy behavior is devoid of exploitation, but a tool prevents mental stress on either member of the relationship and buildsecurity18. For instance, an intellectually handicapped individual is prone to exploitation, yet capable of having a healthy sexual behaviour to build safe, constructive sexual expression and healthy relationships, if appropriately empowered with behavioural knowledge23–25.
A person with healthy sexual behaviour esteems herself/ himself and exhibits self-control, whilst being able to indulge in pleasurable sensual and sexual activities. For instance, people with higher self-esteem are less likely initiate sex26,27. Self-esteem in in sexual behaviour transcends self-worth and sexual self-concept. It is attitudinal and a reflection of mental ability28.
In relation to education, a healthy sexual behaviour is characterized by knowledge of the consequences of different forms of sex and sexual activities. For instance, oral sex is associated with risk of preventable infections29; including HIV per se. Adopting the knowledge is attitudinal vis-àvis a behavioural change wheel30–32.Hence the required healthy sexual behaviour is adopting a HIV prevention consciousness that being sexually healthy enough to engage in oral sex requires having a healthy oral cavity33, as well as the HIV-negative and/or positive partner taking medicine34. Other educational characteristics of healthy sexual behaviour include comprehending the impact of media messages and understanding that the drive for sex is powerful and can be integrated into one’s life in positive and healthy ways20.
Considering values, a healthy sexual behaviour involves their identifying or standing by practices that is “right” on the basis of both personal and sociocultural values, which may include compromise, self-control or tolerance. This also includes issues on use contraception to avoid unplanned pregnancy or sexually transmitted disease21.Values may also encompass spirituality20. For instance, religious people abstain from sexual intercourse during their time of ‘prayer and fasting’. Hence, it has been advocated as possible approach to HIV prevention35.
Risky Sexual Behaviours
Risky sexual behaviours can be defined or determined by the level of potential negative outcome36–38. Some authors have defined it as behaviours that increase risk of STD or unwanted pregnancies, especially being in a sexual relationship in early teenage years i.e., before being matured enough to understand the concepts of healthy relationship – is acknowledged as a risky sexual behaviour39. Common examples of risky sexual behaviour include unprotected intercourse, sexual promiscuity and sex involving unwanted pregnancy40. Other sexual behaviours considered inappropriate or unhealthy include inappropriate sexual exposure such as the concept of pedophile, engaging in sexual behaviours in public or with animals, and precocious sexual gestures amongst others19.
It is believed that young people hardly need education to engage in sexual behaviour as it is normal physiological response to puberty. Nevertheless, it is known that certain factors encourage sexual activities that constitute risky or unhealthy sexual behavior7–10. For instance, fashion has been a paradoxical feature in sexuality and attractiveness. While a shoddily dressed person may unattractive or unsexy, the attractively dressed person may be viewed as inappropriate and seductive in certain situations. This is essentially based on the fact that appearance objectifies a person as well as forms the basis of attractiveness and sexual appeal. Importantly, it is acknowledged that unachieved level of attractiveness can lead to unhealthy behavior41. Associated with this social trend are peer-sociocultural pressures to engage in premarital sex11. In this narrative, focus is henceforth on unprotected sexual intercourse as a risky sexual behaviour.
Contraception
Contraception, which is otherwise known as birth or fertility control, has been defined as the deliberate prevention of conception. It has been used since ancient times- e.g., Egyptian Ebers Papyrus involving use of honey and acacia was adopted in the first century42, but safer methods probably became available in the 20th century43. There are up to fifteen methods of contraception that can be grouped into two broad types, which includes barrier and hormonal methods44. The barrier methods such as condoms and diaphragm help to protect against pregnancy as well as Sexually Transmitted Infection (STI), while hormonal methods prevent pregnancy, only.
Beside the barrier and hormonal methods, there is also the behavioural methods45,46. This includes sexual abstinence that is the most effective preventing pregnancy as well as STI46. Another behavioural method of contraception is coitus interruptus that has a failure rate similar to barrier methods. Other behavioural methods include fertility awareness, lactational amenorrhea and natural family planning amongst others.
Determinants of the Choice and Use of Contraceptive
The schematic presentation in Figure 1 examines the relative roles of individual and social support factors as determinants of the use of contraceptive and choice of methods. Determinants are divided into four general classes: 1. Demand-generating factors such as education, age and other personal characteristics; 2. Demand components which are composed of desire to limit births and desire to space future births 3. Supply factors and 4. Demand crystallising components which are composed of factors that facilitate the implementation of the outcome such as spousal support, peer/social support and parental support (Figure 2)47,48.

In this framework, programme activities play a role in contraceptive method adoption that is similar to the roles of social, familiar and spousal support. The psychological, logistical and social constraints to contraceptive adoption are offset by programme activities that enhance service accessibility, improve the climate of information exchange and legitimise contraceptive behaviour13,49.
Use of Contraception
Contraceptive usage is the percentage of women (and/or sexual partner) that is currently using at least any one of the methods of contraception. According to the World Health Organization, it is based on women within the age range of 15-49 years old. It has been estimated that globally54; about 60% married women of child-bearing age are using contraception, but the frequency of usage of the different methods varies widely between countries (Table 1).
| Contraceptive method | LMIC overall† | Nigeria‡ |
|---|---|---|
| Condom | 11 | 26.6 |
| Oral pill | 12 | 1.6 |
| Intra uterine device | 30 | 0.6 |
| Abstinence | 3.6 | 5.8 |
| Female sterilization | 35 | NR |
| Male sterilization | 4 | NR |
| Withdrawal | NR | 6.4 |
Not with standing the figures indicated on Table 1, other reports have suggested that most common method in the developed world is condoms and oral contraceptives, while in Africa it is oral contraceptives52.Contraceptive use among women in sub-Saharan Africa has risen from about 5% in 1991 to about 30% in 200650, which means a reduction in unmet needs. Yet, comparison of contraceptive usage in sub-Saharan Africa, especially West Africa leaves much to be desired when compared to the world’s average (Figure 3). Of particular note is that less than 20% of Nigerian women are using any method of contraception53.
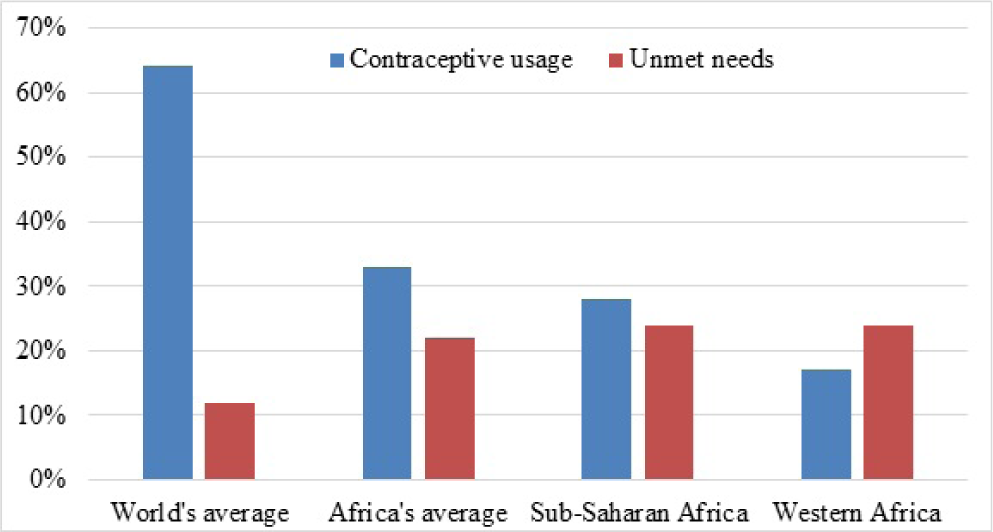
- Contraceptive usage and unmet needs in West Africa relative to world’s average53.
In Nigeria, various studies show the pattern of contraceptive usage. In a study of 500 youth participants51, only 34.2% claimed to have used contraceptives out of which a vast majority used condoms (Table 1). Another report about Nigerian women aged 15-49 in the period of 1981 to 2013 is presented graphically in Figure 4.

- Contraceptive usage in Nigeria during 1981-201354.
Knowledge and Usage of Contraceptive among University Students
The result of the study on contraceptive knowledge and usage among female secondary schools in Lagos State, showed that 5% of 1155 students with knowledge of contraception are users of contraception, 85% of sexually active respondents were non-users while condom is the most common contraceptive method used49. This data regarding condom usage is in agreement with the report from Abuja presented in Table 1.
It has been found that most of the students have knowledge of contraception, but the rate of contraception use is still low17. Yet, it is suggested that the depth of the knowledge may be poor or just fair22, and probably dependent on parental socioeconomic status55. It was argued:
Parents’ levels of education and income are significant predictors of a student’s use of contraceptives.
The students from low socioeconomic background are less likely to use contraceptives is low, especially where the contraceptives are neither free of charge, nor readily available.
Thus, there may be issue of behavioural change wheel vis-à-vis capacity, motivation and opportunity surrounding the unmet needs of family planning among undergraduate students. This probability of behavioural change wheel is supported by reports of other studies indicating that socioeconomic background to students influences their access to and use of contraceptives56–58. Perhaps, what seems to be missing in the discourse is that pregnancy rates among the girls in university community is apparently very low, which is indicated by a highly maintained uninterrupted education. Whether abortion rate is higher (compared to non-students subpopulation) is unknown.
Further from a study conducted in Delta State of Nigeria, there is a negative attitude towards the use of contraceptives with a good fraction of people explaining either that it interferes with pleasure during sex, or they just would not use condoms in sexual relationships with trusted partners5. This also hinges on behavioural change wheel, but it is of different perspective from socioeconomic status factor. For instance, non-users influenced by low socioeconomic status may become users, if given the affordance/capacity, whereas those with negative attitude may already have the capacity but lack motivation. This does not explain the apparent success in pregnancy prevention among female students, though.
Implication for Further Studies
There is a plethora of research that has been going on to improve ‘Family Planning Methods and Services’ (FPMS). A cursory search of PubMed, alone, for FPMS, yields thousands of published articles including hundreds arising from any single Low-Mid Income Country (LMIC). Several factors, methods and programs are already known including but not limited to ideas such as behavioural change motivation21,59, getting closer to the people60, and family education61. Other issues of barriers, generational change and provider behaviour have also been identified62,63. Yet, there is still the problem of unmet needs, which seems to be confounded by the mix-up of sexual behaviour vs sexual health. For instance, erectile dysfunction is a state of being sexually unhealthy and constitutes a sexual health issue that may be helped with a healthy sexual behaviour. A young married man suffering erectile dysfunction can be treated with aphrodisiac64. Evaluation of sexual behaviour, knowledge and the frequency of usage of contraceptive as well as the behavioural change wheel of undergraduate university community will be one step in this direction. The knowledge of how the undergraduate students are handling their contraception in order to maintain uninterrupted education will help in propagating the prevention of sexually transmitted diseases and unwanted pregnancy.
Conclusion
Among the undergraduate students, the prevailing studies have been on first sexual intercourse among undergraduate student, the level of awareness of contraceptives at first intercourse and if being un undergraduate student comes with higher level of awareness; it may be useful to re-evaluate 1. Whether the use of contraceptive by undergraduate students in Delta State differ by age, gender, level of study, religion or marital status; and 2. If the knowledge of contraceptives by the students influences their sexual behavior. These investigations could identify the unmet needs of family planning.
There is also the need to differentiate being sexually healthy from a healthy sexual behaviour. These two phrases seem to be used interchangeably, but it is pertinent they are differentiated. In our opinion, being sexually healthy or unhealthy relates to ability, whereas healthy or risky sexual behaviour is about ‘how’ attitude. That is, Sexual health relates to an underlying pathophysiology that impacts negatively on sexual activity; whereas in healthy sexual behaviour relates to attitude.
References
- Teenage pregnancy and prevalence of abortion among in-school adolescents in North Central, Nigeria. Asian Social Science. 2011;7(1):122.
- [CrossRef] [Google Scholar]
- Physical and neurobehavioral determinants of reproductive onset and success. Nature Genetics. 2016;48(6):617-23.
- [CrossRef] [PubMed] [Google Scholar]
- Determinants of sexual and dating behaviors among adolescents. J Pers Soc Psychol. 1986;50(2):428-38.
- [CrossRef] [PubMed] [Google Scholar]
- Pre-marital sexual debut and its associated factors among in-school adolescents in eastern Ethiopia. BMC Public Health. 2012;12:375.
- [CrossRef] [PubMed] [Google Scholar]
- Knowledge, perception and practice of contraception among staff and students in a university community in Delta State, Nigeria. UK J Pharm and Biosci. 2016;4(1):71-81.
- [CrossRef] [Google Scholar]
- Teenage pregnancy, a worldwide proble. Ned Tijdschr Geneeskd. 2003;147(47):2320-5.
- [PubMed] [Google Scholar]
- Contraceptive behaviors in adolescents. Pediatric Annals. 2005;34(10):794-802.
- [CrossRef] [PubMed] [Google Scholar]
- Adolescent use of contraceptives. NAACOGS Clin Issu Perinat Womens Health Nurs. 1992;3(2):199-208.
- [PubMed] [Google Scholar]
- A reconsideration of sex differences in response to sexual and emotional infidelity. Arch Sex Behav. 2014;43(7):1281-8.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence of premarital sexual practice and associated factors among undergraduate health science students of Madawalabu University, Bale Goba, South East Ethiopia: institution based cross sectional study. The Pan African Medical Journal. 2015;20:209.
- [CrossRef] [PubMed] [Google Scholar]
- Contraceptive knowledge, sexual behavior, and factors associated with contraceptive use among female undergraduate university students in Kilimanjaro region in Tanzania. Adolesc Health Med Ther. 2016;7:109-15.
- [CrossRef] [PubMed] [Google Scholar]
- Sexual experience affects reproductive behavior and preoptic androgen receptors in male mice. Hormones and Behavior. 2012;61(4):472-8.
- [CrossRef] [PubMed] [Google Scholar]
- Defining sexual health: A descriptive overview. Arch Sex Behav. 2004;33(3):189-95.
- [CrossRef] [PubMed] [Google Scholar]
- Sexual activity, contraceptive use, and childbearing of teenagers aged 15-19, in the United States. NCHS Data Brief. 209:1-8.
- [Google Scholar]
- Sexual behaviour, contraceptive knowledge and use among female undergraduates' students of Muhimbili and Dar es Salaam Universities, Tanzania: A cross-sectional study. BMC Women's Health. 2014;14(1):94.
- [CrossRef] [PubMed] [Google Scholar]
- Using behavior change communication to lead a comprehensive family planning program: The Nigerian Urban Reproductive Health Initiative. Glob Health Sci Pract. 2014;2(4):427-43.
- [CrossRef] [PubMed] [Google Scholar]
- Sexual behaviour, contraceptive knowledge and useamongfemale undergraduates in tertiary institutions in Imo State, Nigeria. American Journal of Medical Sciences and Medicine. 2015;3(5):61-6.
- [Google Scholar]
- Sexual health for people with intellectual disability. Salud Publica Mex. 2008;50(Suppl 2):s255-9.
- [CrossRef] [PubMed] [Google Scholar]
- Intellectual disability, sexuality and sexual abuse prevention-A study of family members and support workers. Aust Fam Physician. 2012;41(3):135-9.
- [PubMed] [Google Scholar]
- Sexuality and sex education of adolescents with intellectual disability: mothers' attitudes, experiences, and support needs. Intellect Dev Disabil. 2012;50(2):140-54.
- [CrossRef] [PubMed] [Google Scholar]
- Self-esteem, emotional distress and sexual behavior among adolescent females: Inter-relationships and temporal effects. J Adolesc Health. 2006;38(3):268-74.
- [CrossRef] [PubMed] [Google Scholar]
- Personality and riskier sexual behaviour: Motivational mediators. Psychology and Health. 2007;22(3):291-315.
- [CrossRef] [Google Scholar]
- The relationship between self-esteem and sexual self-concept in people with physical-motor disabilities. Iran Red Crescent Med J. 2015;17(1):e25359.
- [CrossRef] [PubMed] [Google Scholar]
- Oral sex, oral health and orogenital infections. J Glob Infect Dis. 2010;2(1):57-62.
- [CrossRef] [PubMed] [Google Scholar]
- Hierarchical multiple regression modelling on predictors of behavior and sexual practices at Takoradi Polytechnic, Ghana. Glob J Health Sci. 2015;7(4):200-10.
- [CrossRef] [PubMed] [Google Scholar]
- Attitudinal changes using peer education training in the prevention of HIV/AIDS: A case study of youths in North Central Nigeria. Adv Pharm Bull. 2013;3(1):45-50.
- [PubMed] [Google Scholar]
- Systematic review: A review of adolescent Behavior Change Interventions [BCI] and their effectiveness in HIV and AIDS prevention in sub-Saharan Africa. BMC Public Health. 2017;17(1):718.
- [CrossRef] [PubMed] [Google Scholar]
- Oral sex and oral health: An enigma in itself. Indian J Sex Transm Dis. 2015;36(2):129-32.
- [CrossRef] [PubMed] [Google Scholar]
- Religiosity for HIV prevention in Uganda: A case study among Muslim youth in Wakiso District. Afr Health Sci. 2012;12(3):282-90.
- [CrossRef] [PubMed] [Google Scholar]
- Sexual activity and contraceptive use among young female students of tertiary educational institutions in Ilorin, Nigeria. Contraception. 2009;79(2):146-9.
- [CrossRef] [PubMed] [Google Scholar]
- Pregnancy in adolescents. Adolesc Med State Art Rev. 2012;23(1):123-38.
- [CrossRef] [PubMed] [Google Scholar]
- The social context for risky sexual behavior among adolescents. J Behav Med. 1994;17(4):419-38.
- [CrossRef] [PubMed] [Google Scholar]
- Teenage pregnancy rates and associations with other health risk behaviours: A three-wave cross-sectional study among South African school-going adolescents. Reproductive Health. 2016;13:50.
- [CrossRef] [PubMed] [Google Scholar]
- The relationship between sexual abuse and risky sexual behavior among adolescent boys: A meta-analysis. J Adolesc Health. 2012;51(1):18-24.
- [CrossRef] [PubMed] [Google Scholar]
- Reproduction concepts and practices in ancient Egypt mirrored by modern medicine. Eur J Obstet Gynecol Reprod Biol. 2005;123(1):3-8.
- [CrossRef] [PubMed] [Google Scholar]
- Fertility control in man: the history of contraception from antiquity to the present. Lakartidningen. 1977;74(51):4598-600.
- [PubMed] [Google Scholar]
- The use of behavioral methods of contraception in women seeking abortion. N Z Med J. 1997;110(1054):393-5.
- [PubMed] [Google Scholar]
- Behavioral Methods of Contraception In: Shoupe D, Kjos SL, eds. The handbook of contraception, A guide for practical management. Totowa, NJ: Humana Press; 2006. p. :179-94.
- [Google Scholar]
- Contraceptive use among young women in Namibia: Determinants and policy implications: University of Namibia 2008.
- [Google Scholar]
- Determinants of contraceptive use among Nigerian couples: Evidence from the 2013 Demographic and Health Survey. Contraception and Reproductive Medicine. 2017;2(1):9.
- [CrossRef] [Google Scholar]
- Contraceptive knowledge and usage amongst female secondary school students in Lagos, Southwest Nigeria. Journal of Public Health and Epidemiology. 2011;3(1):34-7.
- [Google Scholar]
- Family planning in sub-Saharan Africa: Progress or stagnation? Bulletin of the World Health Organization. 2011;89(2):137-43.
- [CrossRef] [PubMed] [Google Scholar]
- Trends in contraceptive need and use in developing countries in 2003, 2008 and 2012: An analysis of national surveys. The Lancet. 2013;381(9879):1756-62.
- [CrossRef] [Google Scholar]
- Trends in contraceptive use worldwide 2015. Department of Economic and Social Affairs, Population Division. ST/ESA/SER.A/349
- [Google Scholar]
- World contraceptive use 2017. Department of economic and social affairs, population division. POP/DB/CP/Rev2017
- [Google Scholar]
- Knowledge and use of contraceptives among tertiary education students in south africa. Mediterranean Journal of Social Sciences. 2014;5(10):500.
- [CrossRef] [Google Scholar]
- Self-concept and locus of control as correlates of reproductive health knowledge of students in Nigerian universities. The Social Sciences. 2008;3(2):88-95.
- [Google Scholar]
- An examination of university students' attitude to contraceptive use. American International Journal of Social Science. 2013;2(1):18-22.
- [Google Scholar]
- Contraception and Unintended pregnancy among unmarried female university students: A cross-sectional study from China. PLoS One. 2015;10(6):e0130212.
- [CrossRef] [PubMed] [Google Scholar]
- Motivations and constraints to family planning: A qualitative study in Rwanda's Southern Kayonza District. Glob Health Sci Pract. 2015;3(2):242-54.
- [CrossRef] [PubMed] [Google Scholar]
- Integrating population, health, and environment programs with contraceptive distribution in rural Ethiopia: A qualitative case study. Stud Fam Plann. 2015;46(1):41-54.
- [CrossRef] [PubMed] [Google Scholar]
- Couple based family planning education: changes in male involvement and contraceptive use among married couples in Jimma Zone, Ethiopia. BMC Public Health. 2015;15(1):682.
- [CrossRef] [PubMed] [Google Scholar]
- Predictors of modern contraceptive use during the postpartum period among women in Uganda: a population-based cross sectional study. BMC Public Health. 2015;15(1):262.
- [CrossRef] [PubMed] [Google Scholar]
- Determinants of maternal health services utilization in Uganda. BMC Health Serv Res. 2015;15(1):271.
- [CrossRef] [PubMed] [Google Scholar]
- A review of the potential of medicinal plants in the management and treatment of male sexual dysfunction. Andrologia. 2016;48(8):880-93.
- [CrossRef] [PubMed] [Google Scholar]




