
Translate this page into:
Role of Periodontal Evaluation in Tooth Supported Overdenture
*Email: drkamattoo@rediffmail.com
Abstract
Preventing a prosthodontic situation is subjective in nature and different views exist, but the principle remains same. Periodontal evaluation before commencing treatment and during follow up cannot be undermined by any means. The use of overdenture allows an individual to retain the roots of natural teeth, which by any mean are the best option to preserve the residual alveolar ridge. We present a case of an elderly patient who presented with supraerupted and rotated maxillary and mandibular anterior teeth. Four maxillary and three mandibular anterior teeth were retained and after endodontic treatment of each, a dowel post with the ball attachment was customized to fit the ‘O’ ring placed within each denture.
Keywords
Attached Gingiva
Cast Restoration
Dowel
Post Space

Introduction
The importance of retaining natural teeth goes far beyond esthetics and mastication when it comes to predicting the future of complete edentulism. The concept of overdenture as a viable treatment started in 1960’s, and continues to be practiced globally on the same principles1–3. The retention of roots within the alveolar bone preserves its form besides minimizing the vertical and lateral movements of the denture. The biologic advantage of retaining the natural tooth remains when a tooth is kept within the bone. Advancement in overdenture treatment over the last few decades has only been related to placement of implant within the alveolar bone on which an overdenture is fabricated. However, even implant supported overdenture has less advantages than a natural tooth retained overdenture4,5.
The tooth supported overdenture is a conservative and preventive treatment modality of prosthodontics that depends largely on the periodontal prognosis of the abutment teeth that it derives support from. Most of the prosthodontist under normal circumstances do not consult a periodontist at times. Periodontal screening in such cases is beyond plaque control or hygiene maintenance. The main goal for any tooth supporting a prosthesis is to diagnose periodontal condition that could compromise future of the prosthesis6. A tooth that is not properly inclined in the arch itself is a potential candidate for periodontal disaster. Whenever, tilted, rotated, angulated or supraerupted teeth are used as an abutment either for a removable or for a fixed partial denture, the periodontal screening should be a part of the treatment protocol. Not only is the oral hygiene crucial in such cases, but some of the teeth may require definitive periodontal treatment also7. This article in the form of a case report presents rehabilitation of a completely edentulous patient who received both maxillary and mandibular tooth supported overdenture. All the abutment teeth were not ideally inclined and therefore a thorough periodontal screening was an essential part of the treatment plan.
Case Report
An elderly male patient aged 67 years reported to the department of prosthodontics seeking replacement of his missing teeth. Medical, social, drug history was non-contributory. Dental history revealed frequent extraction of mobile teeth over last ten years. Extra oral examination presented normal features except increased lower third of the face (Figure 1a). Intra oral picture was that of presence of supraerupted, tilted or rotated maxillary and mandibular anterior teeth. Almost all of the teeth had an accumulation of plaque beneath the undercut that was formed as a result of change in their respective axial inclinations. A thorough periodontal screening was requested which disclosed necessity of definitive periodontal treatment in relation to maxillary and mandibular teeth.

- (a) Extra oral view of the patient showing increased lower third of the face (b) Intraoral view showing remaining natural teeth (c) Remaining teeth after endodontic treatment (d) O ring (e) Wax pattern engulfing a premachined plastic precision attachment.
After a periodontal maintenance phase, clinical and radiographic investigation for prosthetic treatment was done. Treatment options suggested to the patient was overdenture as first choice, the immediate denture as second and conventional complete denture after extraction of all teeth as third choice. The patient consented for overdenture prosthetic option for which four maxillary anterior and three mandibular anterior teeth were selected to be retained while the rest were indicated for extraction. Treatment planning for overdenture included periodontal reevaluation and extraction of undesired teeth, which were later to be followed by endodontic treatment of planned teeth. The preparatory phase finished by the second month after diagnosis and treatment plan stage. Overdenture fabrication started by first preparing the remaining natural teeth extracoronally followed by intra radicular preparations (Figure 1b) to allow placement of prefabricated plastic precision attachment that would be attached to the denture with O ring attachments. After the clinical procedure for tooth preparation was done (Figure 1c), a definitive impression using elastomeric impression material (Reprosil, Dentsply/Caulk; Milford, DE, USA) was made which included an impression of the radicular prepared spaces of all teeth. The working cast for both maxillary and mandibular denture was prepared using Type IV dental stone (Ultrarock, Kalabhai Dental, India) and preformed plastic forms (Bredent attachment systems, USA) were inserted and modified for each abutment tooth. Each plastic form was to be retained by an ‘O’ ring (Figure 1d) which would engage a ball pin head of the cast plastic form (Figure 1e).
The modified plastic forms for all designed abutment teeth were then cast into the base metal alloy. Each casting was accurately fitted with the cast (Figure 2a) following which they were cemented into place for each tooth (Figure 2b). The rings for each denture was incorporated directly in the patient’s mouth (Figure 2c) using the patients existing centric occlusion and both dentures were delivered to the patient after educating him about maintenance of dentures. The patient was extremely satisfied with the functional outcome of the prosthesis and did not report any problems during denture adaptation (Figure 2d).
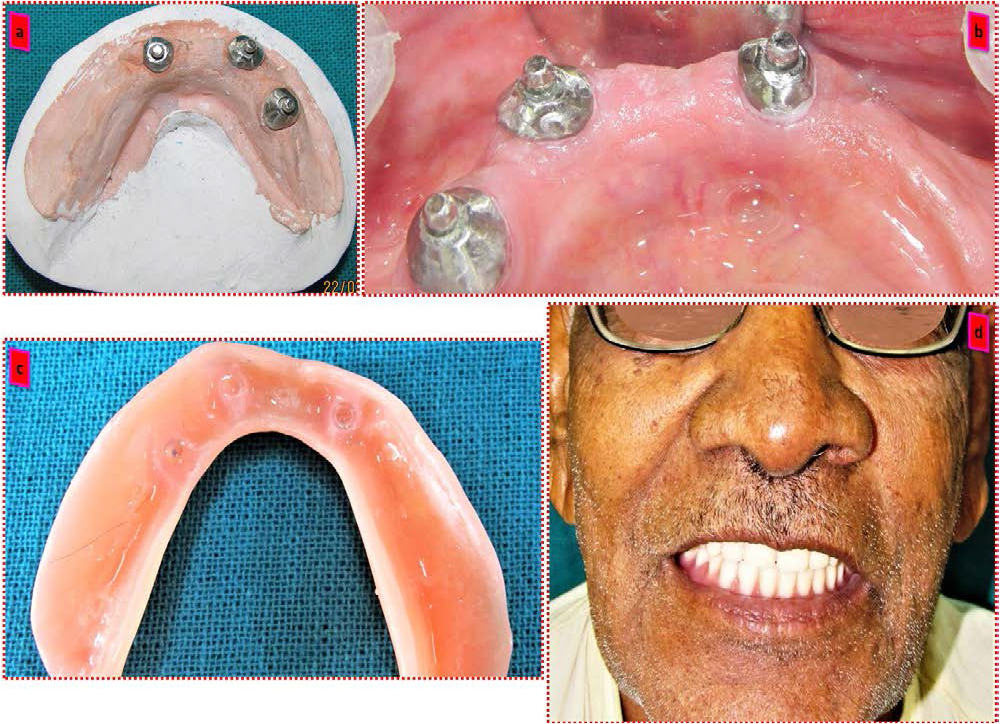
- (a) Cast dowel attachment (b) Cast attachment cemented to remaining roots (c) O ring attached to complete denture (d) Final completed denture.
Discussion
A partial edentulous situation like the one described in this case report is one among the thousands of possible combinations. A patient with few teeth remaining is the ideal choice for having an overdenture although the ideal location of teeth is another important factor in the biomechanics of overdenture prosthesis. Periodontal involvement of the teeth and supraeruption of teeth are two important factors pertaining to the present case that needs to be discussed. The patient reported that most of his natural teeth were lost because they were mobile. Although the mobility of a supraerupted tooth decreases after reducing the height of the tooth, it is important to observe the presence of attached gingiva around the tooth8. Such teeth may not survive for long since they are already unstable. The length of the remaining root that is present within the bone is another important consideration. Any tooth within the realm of grade 1 or grade 2 periodontal mobility can be used for an overdenture abutment provided the presence of attached gingiva is around and there is enough root within the alveolar bone9. If a tooth is mobile and has an adjacent natural tooth present, then the condition is more favourable than when the periodontally involved tooth is isolated10. In relation to individual abutment selection the amount of attached gingiva that is present on the tooth is more important than the actual mobility. Therefore, consideration of the amount of attached gingiva is a better clinical indicator for predicting the prognosis of an abutment tooth. Supraeruption of the tooth is a less likely factor to contraindicate the use of overdenture since supraeruption is corrected once the abutment tooth is prepared till the level of gingiva.
Conclusion
Periodontal screening is an important tool to determine the prognosis of a tooth that supports a prosthesis. a prosthodontist should always ask a periodontal opinion whenever such cases are planned.
Acknowledgement
The authors would like to acknowledge the efforts of the staff of the department of prosthodontics for their valued effort in completing the treatment of this case.
References
- Adaptation and the hybrid prosthesis. Journal of Prosthetic Dentistry. 1955;5:811-23.
- [CrossRef] [Google Scholar]
- Complete dentures supported by natural teeth. Journal of Prosthetic Dentistry. 1958;8:924-8.
- [CrossRef] [Google Scholar]
- Conservation of the supportive mechanism. Journal of Prosthetic Dentistry. 1965;19:327-38.
- [CrossRef] [Google Scholar]
- Tooth supported complete dentures: Description and clinical evaluation of a simplified technique. Journal of Prosthetic Dentistry. 1969;27:414.
- [CrossRef] [Google Scholar]
- An overdenture survey: Preliminary report. Journal of Prosthetic Dentistry. 1977;37:246.
- [CrossRef] [Google Scholar]
- Preparation of mouth for removable partial dentures In: McCracken’s Removable Partial Dentures. ed 8. St Louis: Mosby; 1989. p. :263-5.
- [Google Scholar]
- Periodontal conditions following treatment with distally extending cantilever ridges or removable partial dentures in elderly patients. A 5-year study. Journal of Periodontology. 1990;61:21-6.
- [CrossRef] [Google Scholar]
- The relationship between success of free gingival grafts and transplant thickness. Journal of Periodontology. 1981;52:74.
- [CrossRef] [Google Scholar]
- The ecology of the prosthodontic problem. The Journal of the American Dental Association. 1976;92:133.
- [CrossRef] [Google Scholar]




