
Translate this page into:
Incidental finding of left adnexum agenesis observed at cesarean section: A case report

* Corresponding author: Dr. Mariam Abdulbaki, Department of Obstetrics and Gynecology, Kwara State University Teaching Hospital, Ilorin, Kwara State, Nigeria. pricelessmariam@yahoo.com
-
Received: ,
Accepted: ,
How to cite this article: Abdulbaki M, Gbadeyan R, Aliyu FO, Adeniran AS. Incidental finding of left adnexum agenesis observed at cesarean section: A case report. J Health Sci Res. 2025;10:32-4. doi: 10.25259/JHSR_42_2024
Abstract
Congenital adnexum agenesis is a rare finding with a suggested incidence of 1: 11,240. It is usually associated with infertility and rarely seen in pregnancy. Herein, we presented a detailed case report of this rare occurrence of an incidental finding of left adnexum agenesis with their intraoperative images observed at cesarean section in a Nigerian lady at the Kwara State University Teaching Hospital, Ilorin, Kwara State, Nigeria. This finding was observed during an emergency cesarean section carried out on a 23 year old primigravida at a tertiary healthcare facility in north-central Nigeria. Complete agenesis of the left adnexum with grossly normal uterine body and right adnexum (ovary, fallopian tube and broad ligament) was observed. This is a rare condition incidentally found at cesarean section of an otherwise asymptomatic patient thereby throwing more light on its incidence.
Keywords
Cesarean delivery
Ultrasound
Unilateral broad ligament agenesis
Unilateral ovarian agenesis
Unilateral tubal agenesis

INTRODUCTION
Congenital unilateral agenesis of the adnexum (ovary, broad ligament, and fallopian tube) is a rare anomaly with a few previous reports in the literature.[1,2] The incidence has been difficult to determine accurately due to the rarity, although a report indicated an incidence of 1:11,240 cases.[3] Generally, there is no clear method of diagnosing this condition; most ultrasonography do not check these structures routinely, especially during pregnancy, because the fallopian tubes or ovaries are not usually a priority, except when there are specific indications such as infertility, which may explain its association with infertility. Therefore, most cases are diagnosed incidentally at laparoscopy or laparotomy for a different indication.[4] However, in the case presented, the diagnosis was an incidental finding at cesarean delivery, which has been less reported.[2] The diagnosis at cesarean section is rare given the association of the condition with infertility, thereby necessitating this report.
CASE REPORT
A 23-year-old primigravida was referred from a private hospital at 34 weeks gestational age on account of severe preeclampsia with a blood pressure of 200/140 mmHg taken before referral. There was no drainage of liquor, bleeding per vaginam, uterine contractions, or convulsion. She was married in a monogamous family and had no history of infertility or any previous surgeries.
At the presentation in our facility, the essential findings were that of blood pressure measuring 150/90mmHg, urinalysis on dipstick showed proteinuria of 2+ but negative for blood. She was counseled about her clinical condition and admitted, and samples were taken for investigations including serum electrolyte, urea and creatinine, liver function test, full blood count, and platelet counts. An obstetric ultrasound scan for biophysical profile was essentially normal. She received parenteral dexamethasone for fetal lung maturity and antihypertensive (Nifedipine) for blood pressure control. She however, left the hospital against medical advice while she was being stabilized with a birth plan for a scheduled abdominal delivery.
She presented again after 48 h with an 8-hour history of throbbing headache and blurring of vision, and a 4-hour history of fetal movement absence but no convulsions. On examination, she was not pale, afebrile, or anicteric with bilateral pitting pedal edema. The pulse rate was 100 beats per minute, regular, blood pressure 250/150 mmHg, respiratory rate 22 cycles per minute, and the chest was clear clinically on auscultation. Obstetric examination showed uterine size of 32 cm with no palpable contractions; the fetus was in cephalic presentation, descent was 5/5 palpable, and fetal heart rate was 170 beats per minute. Pelvic examination showed an unripe cervix with a Bishop score of 2, urinalysis showed 3+ protein, clotting time was normal, and hemoglobin concentration was 10 g/dL. She was stabilized with parenteral antihypertensive (Intermittent Hydralazine) and anticonvulsant (magnesium sulfate) with a birth plan for an emergency cesarean section. She received oxygen supplementation with a nasal catheter, a urethral catheter was passed and retained to monitor urine output, and she was delivered via cesarean section.
The intraoperative findings showed a live female neonate with Apgar scores of 41 and 85, respectively, grossly normal uterine body and right adnexum (ovary, fallopian tube and broad ligament) [Figure 1] with complete agenesis of the left adnexum [Figure 2] and estimated blood loss of 800 mL. The postoperative period was not adversely eventful. The blood pressure was well controlled and she was discharged on the fifth day with her baby. She was seen at the 6-week postpartum clinic visit, and both mother and baby were in good health.
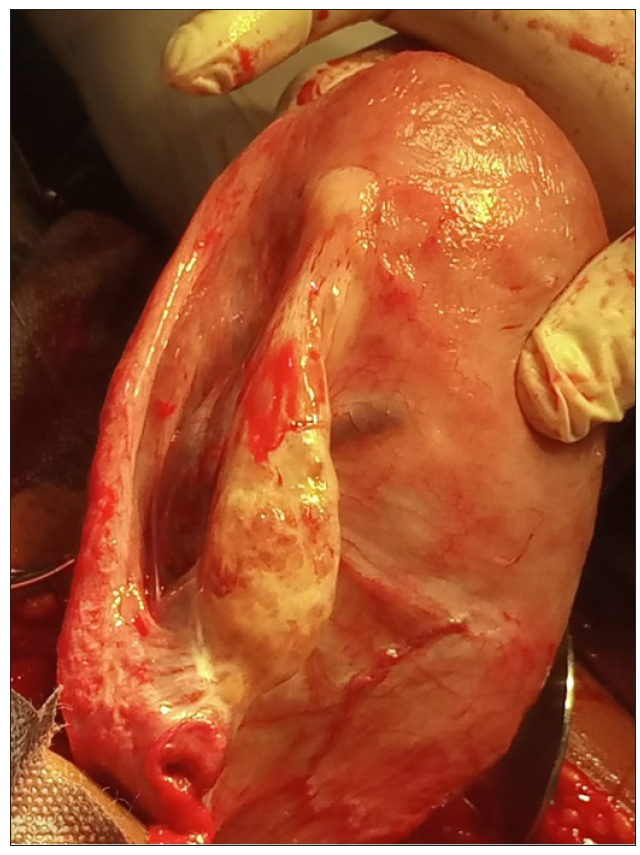
- Shows the presence of the right adnexa and complete agenesis of the left adnexum.

- Shows the absence of the left ovary, fallopian tube, and broad ligament.
DISCUSSION
The case presented was that of a 23-year-old Nigerian lady with no history of previous surgeries or infertility, who had an emergency cesarean delivery on account of severe preeclampsia with an unripe cervix. She delivered a live female neonate with incidental finding of congenital agenesis of the left adnexum and a normal uterine body and right adnexum.
Unilateral absence of the adnexum without uterine abnormality is rare in the literature.[2] The incidence is difficult to determine because a majority of women with this condition are asymptomatic and go unreported[2] although an incidence of 1:11,240 individuals has been reported.[3] Majority of the women were diagnosed incidentally during interventions, that is, laparoscopy or laparotomy performed for a different cause,[2–4] although it has been reported to be associated with infertility.[1–4] The exact etiology of the agenesis of the ipsilateral ovary and/or fallopian tube is yet to be elucidated.[5] It is suggested that it may either be a congenital malformation of the ovarian pedicle at birth, during childhood or adult life, or the result of torsion of the adnexum resulting in ischemia, necrosis, and reabsorption in-utero or postnatal life.[5] Another suggestion focuses on a defect in the development of the entire Müllerian and mesonephric systems on one side or a defect localized to the region of the genital ridge and the caudal part of the Müllerian duct.[5]
The first published case of unilateral agenesis of the adnexum was in 1923,[6] while other cases have been reported recently, possibly due to the increasing use of diagnostic laparoscopy.[3,4] Unlike the case presented, unilateral congenital agenesis of the adnexum has also been associated with concurrent malformations of the uterus and/or the urinary tract, such as unicornuate uterus and unilateral renal agenesis.[7] However, the explanation for the presence or absence of concurrent anomalies aside from the agenesis of the adnexum remains to be established. In all, women without concurrent uterine anomaly stand a higher probability of spontaneous conception and delivery, although they stand to pass unrecognized unless with incidental findings. On the other hand, associated background infertility increases the probability of diagnosis since it requires additional investigative modalities that may aid in the diagnosis.
In addition, this patient had multiple ultrasound scans during pregnancy, but none was able to diagnose the condition. However, anomalies of the fallopian tube can also be diagnosed with hysterosalpingography and laparoscopy.[7] Although ultrasonography can evaluate the external contour of the uterus and adnexum and can diagnose fetal congenital anomalies,[8] it is not routinely used to diagnose congenital anatomical anomalies of the uterus during pregnancy. In addition, a pelvic CT scan can also be used, which however is limited to nonpregnant women. Several cases reported were associated with infertility and were diagnosed from clinical workup with hysterosalpingography showing occlusion of the affected fallopian tube and a follow-up laparoscopic evaluation showing an absent adnexa.[2–4]
Therefore, it is worthwhile to consider assessment of other pelvis organs during imaging in non-pregnant and pregnant women to provide a holistic picture of the reproductive anatomy.
CONCLUSION
This case is an addition to the few reported cases of incidental diagnosis of agenesis of the adnexum diagnosed at cesarean section despite multiple antenatal ultrasound scan evaluations. This case report further highlights the need to consider routine assessment of other pelvic structures during routine pelvic ultrasonography in nonpregnant and pregnant women.
Authors’ contributions
AM: Concept, design, data collection, data interpretation, drafting, critical appraisal and approval of the final manuscript; FOA: Concept, design, data collection, data interpretation, drafting and approval of the final manuscript; GR: Concept, design, data interpretation, drafting, and approval of the final manuscript; AAS: Concept, design, data interpretation, drafting, and approval of the final manuscript.
Ethical approval
The research/study was approved by the Institutional Review Board of the Kwara State University Teaching Hospital, number KWASUTH/IRC/246/VOL.II/29, dated October 02, 2024.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
REFERENCES
- Incidental finding of unilateral partial agenesis of fallopian tube with complete agenesis of ipsilateral ovary during cesarean section with neonatal outcome. Int J Reprod Contracept Obstet Gynecol. 2023;12:1941-3.
- [Google Scholar]
- Unexplained unilateral absence of ovary and fallopian tube. Eur J Obstet Gynecol Reprod Biol. 1986;22:103-5.
- [CrossRef] [PubMed] [Google Scholar]
- Unilateral ovarian agenesis incidentally diagnosed by laparoscopy. Ame J Surg Clin Case Rep. 2022;4:1-3.
- [Google Scholar]
- The overview of anatomical variations and congenital anomalies of the uterine tubes and their impact on fertility. Physiol Res. 2022;71:S35-49.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- True unicornuate uterus and total absence of left broad ligament, round ligament, salpinx, ovary, kidney and ureter. Can Med Assoc J. 1947;56:539.
- [Google Scholar]
- Ovarian absence: A systematic literature review and case series report. J Ovarian Res. 2023;16:13.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Congenital anatomical variants in human fetal embryological development and its risk factors in low-resource setting: A longitudinal study. J Health Sci Res. 2024;9:1-6.
- [Google Scholar]




